Publication
Article
Demystifying the Role of Palliative Care in the Oncology Clinic
In Partnership With:


Despite American Society of Clinical Oncology guidelines calling for introduction of palliative care early in the course of disease, these services remain underused.


Laura Shoemaker, DO

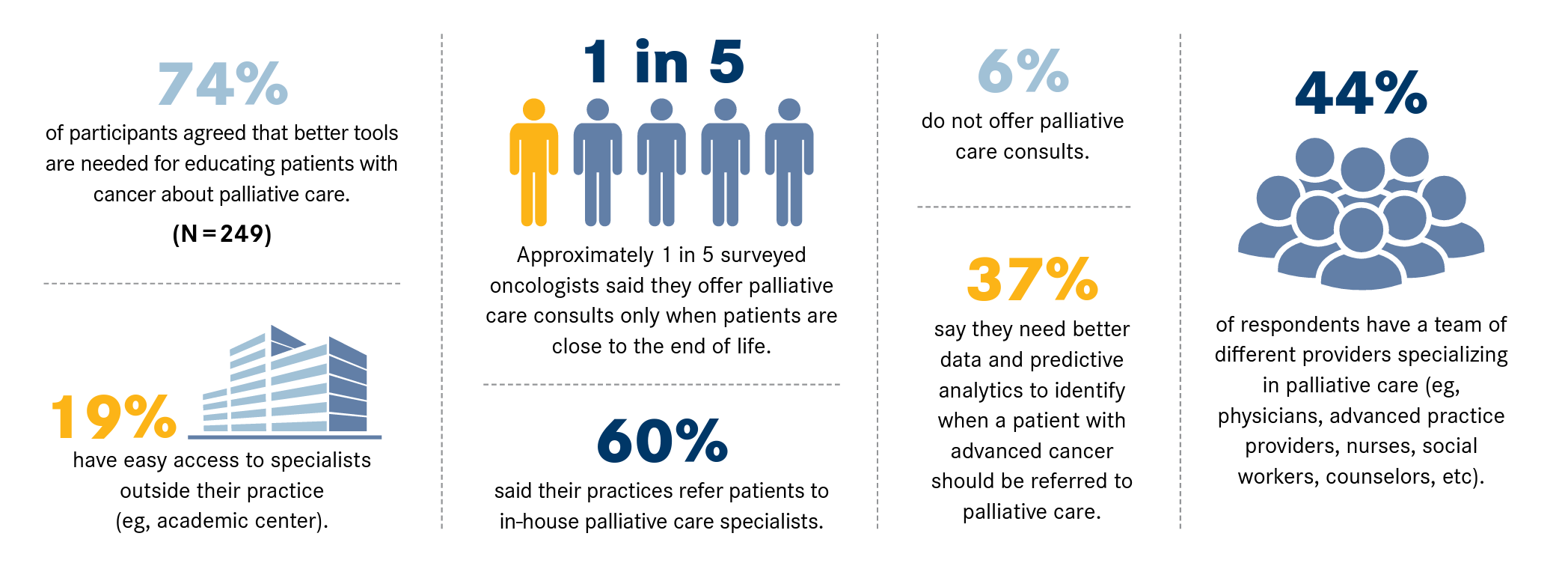
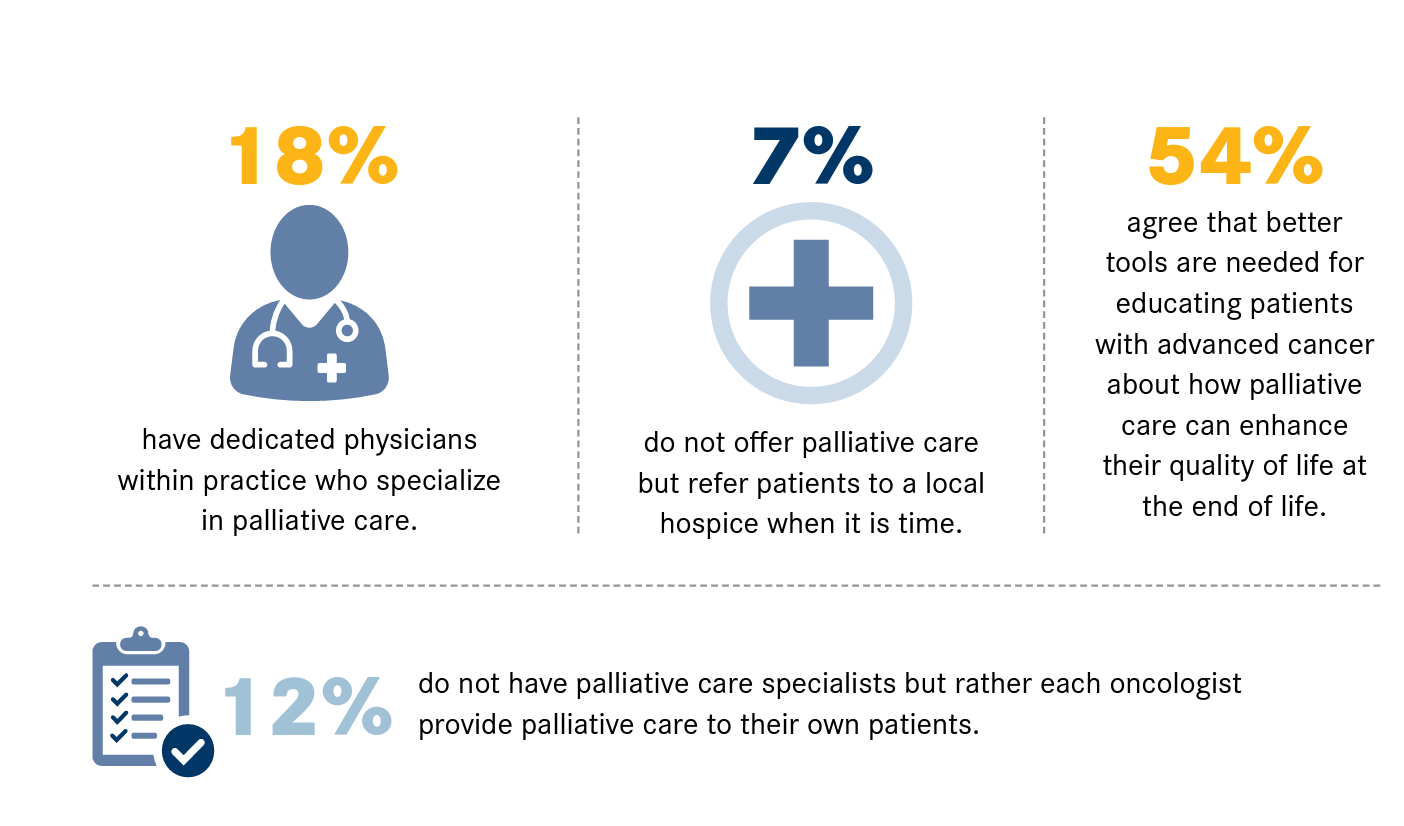
Despite American Society of Clinical Oncology guidelines calling for introduction of palliative care early in the course of disease, these services remain underused.1 A recent survey of 249 oncologists nationwide found only 26% made palliative care referrals for patients on active treatment.2
One barrier to introducing palliative care is lack of understanding about exactly what these services entail and how to talk about them with patients (Figure).2 Palliative care is specialized care to help relieve symptoms and stress for anyone living with a serious illness. Specialized palliative care physicians, advanced practice registered nurses, and social workers offer an additional layer of support to any patient with serious disease, no matter where they are in their health journey.


Figure. Challenges to Palliative Care Integration in Oncology Care2
“Palliative care can be applied early in the trajectory of serious illness and aligns with a plethora of goals that include everything from cure to life prolongation,” Laura Shoemaker, DO, says. Shoemaker is chair of the Department of Palliative and Supportive Care at Cleveland Clinic in Ohio. “The focus is on living as well as possible and improving the quality of life for both patients and families.”


Figure. Challenges to Palliative Care Integration in Oncology Care2
Distinguish Palliative Care From Hospice Care
Palliative care is appropriate at any age and any stage in a serious illness and is provided along with curative and disease-modifying therapies. However, even in the medical community, it is not uncommon for individuals to conflate palliative care with hospice care, and this confusion can hinder patients’ ability to receive the added support they need. Physicians may be unclear on how to explain the benefits of palliative medicine or fear that patients will think it means their situation is dire.
“Lacking the right language to introduce palliative care can be a barrier,” Shoemaker says. “Often if they lack better language, physicians will tell a patient they need palliative care, adding, ‘Don’t worry, it’s not hospice.’ This is the least effective way to describe palliative care. How you describe it is vitally important, because if we don’t accurately describe what it is and how it aligns with the patient’s goals and values, they aren’t going to accept it.”
Listen First
Physicians should talk about what palliative care is and not what it isn’t, Shoemaker advises. “It’s helpful to ask questions f irst and tell last,” she says. “So instead of starting the conversation [by] saying you think they need palliative care, ask how they’re coping. For example, ‘I see that you’ve just [received a] diagnosis of cancer and are planning to start chemotherapy and radiation. What is top of mind for you as you start treatment?’” Inquiring first can help uncover physical symptoms such as pain or nausea and psychosocial issues such as sleep disorders. From there, the clinician can have a conversation about extra support available to optimize quality of life and cancer-directed therapies through palliative medicine.
Determine Timing
The right time for introducing palliative care is when a patient with a serious illness experiences a significant functional or caregiving issue. Physicians sometimes assume that palliative care is prognostically limited, but that is not the case. In fact, some patients receive palliative care for years. For others, palliative care is an important part of undergoing treatment or recovering from a serious illness.
Work in Partnership
Palliative medical practitioners take a holistic approach to relieve pain and discomfort and address other challenges that are equally meaningful to that patient and their family. This support adds to the care being provided by the patient’s existing medical team. When the palliative care team sees a patient in the clinic, they can offer support that aligns with the patient’s treatment plan and do a deep dive into symptom management, addressing physical, emotional, and social issues in addition to other issues.
The need for palliative care is likely to increase in the coming years. The emergence of novel therapies means more patients are living longer with cancer, but that does not spare them from the myriad of physical and emotional challenges that accompany the disease.
“Getting a diagnosis of cancer turns your world upside down,” Shoemaker says. “There’s so much going on in a patient’s mind. How will this change my life? Will I be able to keep working? How will I get to appointments? Each conversation is different in terms of what supports a patient’s needs as they embark on treatment.”
Clinicians looking to learn more about palliative medicine or how to educate their patients about it may visit getpalliativecare.org.
Laura Shoemaker, DO, is chair of the Department of Palliative and Supportive Care at Cleveland Clinic in Ohio and vice chair of the Ohio Department of Health’s Palliative Care and Quality of Life Interdisciplinary Council.
References
- Smith CB, Phillips T, Smith TJ. Using the new ASCO clinical practice guideline for palliative care concurrent with oncology care using the TEAM approach. Am Soc Clin Oncol Educ Book. 2017;37:714-723. doi:10.1200/EDBK_175474
- Oncology insights December 2021. Cardinal Health. Accessed December 7, 2022. bit.ly/3F9dy5N