Publication
Article
Oncology & Biotech News
BRIM-2 Upholds Benefits Emerging with Vemurafenib in Melanoma
Author(s):
In Partnership With:


In patients with metastatic melanoma, the BRAF inhibitor vemurafenib led to high objective response rates and durable treatment responses.



Antoni Ribas, MD
In patients with metastatic melanoma, the BRAF inhibitor vemurafenib led to high objective response rates (ORRs) and durable treatment responses in an open-label phase II study presented at ASCO 2011 by Antoni Ribas, MD, of the Jonsson Comprehensive Cancer Center at the University of California, Los Angeles.
“A significant number of patients have ongoing responses between 10 and 12 months from the study start,” said Ribas. “Overall survival (OS) is 58% at 12 months. Median OS has not been reached.”
The study was initiated after the highly encouraging phase I results of the drug in 32 patients with a V600E activating mutation in the BRAF gene. In that study, vemurafenib led to a high incidence of tumor regression and an unconfirmed ORR of 81%. This high ORR has since been downgraded to a confirmed ORR of 53%.
The phase II BRIM-2 trial, which enrolled 132 previously treated patients, essentially validated the initial findings of high activity for the novel agent.
Table. Patient Baseline Disease Characteristics
Characteristic
No. (%)
N = 132
Stage at diagnosis
M1a
M1b
M1c
33 (25)
18 (14)
81 (61)
Serum LDH
Normal
Elevated
67 (51)
65 (49)
No. prior therapies
1
2
3
67 (51)
36 (27)
29 (22)
Previous ipilimumab or
tremelimumab
No
Yes
125 (95)
7 (5)
LDH indicates lactate dehydrogenase.
Adapted from Ribas et al. J Clin Oncol. 2011;29(suppl; abstr 8509).
Patients who had received at least 1 prior line of therapy for metastatic melanoma (49% had received 2 or more) received vemurafenib 960 mg PO BID until progression, unacceptable toxicity, or death. The primary endpoint was ORR by independent review.
At a median follow-up time of 10 months, the ORR was 53%, which met the study’s primary endpoint (a target ORR of 30% and lower boundary of 95% confidence interval of at least 20%). Stable disease was noted in 29% of patients, Ribas reported.
In the prespecified exploratory subset analysis, there were no differences in response rates according to age, gender, performance status, stage, number of prior therapies, or receipt of high-dose interleukin-2. Patients with high baseline lactate dehydrogenase (LDH) (>1.5 times upper limit of normal), however, were less likely to respond than those with normal LDH, he reported.
Median progression-free survival (PFS) was 6.7 months. OS was 77% at 6 months and 58% at 1 year. Median duration of response was 6.7 months, but responses are ongoing for as long as a year in many patients. Ribas added that time to response can also be delayed in some patients, even up to 1 year from start of therapy. At this time, 27% of patients are still on study.
The drug was well tolerated, with the most common side effects being arthralgias (58%), skin rash (52%), and photosensitivity (52%). He said that squamous cell carcinomas develop in about 25% of patients, tend to appear within the first 2 months, and are easily managed.
Dose modifications were necessary in 45% of patients; however, the median daily dose— 1750 mg—was 91% of the intended total dose. Only 4 patients discontinued due to drugrelated adverse events.
Figure. Tumor Response by Independent Review Committee


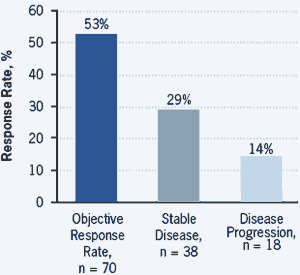
Adapted from Ribas et al. J Clin Oncol. 2011;29(suppl; abstr 8509).
Ribas concluded by noting that the study “complements the observation of benefit seen in BRIM-3” in previously untreated metastatic patients. (This was reported at the ASCO meeting in abstract LBA4.) He said, “Together the results provide evidence that vemurafenib is an effective agent for the treatment of patients with BRAF V600E -positive metastatic melanoma.”
Gary K. Schwartz, MD, chief of the melanomasarcoma service at Memorial Sloan-Kettering Cancer Center in New York, said, “The findings suggest vemurafenib is highly active in BRAF-mutated melanoma but is probably not quite as active as shown in the published phase 1 data.”
“What we have learned from BRIM-2,” said Schwartz, is that patients with elevated LDH do “quite poorly,” with only one-third of patients responding.
He also pointed out that the median duration of response, about 6 months, indicates that “the onset of drug resistance remains a serious concern with this class of drugs, and understanding drug resistance will be critical in drug development.”
Ribas A, Kim KB, Schuchter LM, et al. BRIM-2: an openlabel, multicenter phase II study of vemurafenib in previously treated patients with BRAF V600E mutation-positive metastatic melanoma. J Clin Oncol. 2011;29(suppl; abstr 8509).




































