Publication
Article
Oncology Business News®
NCCN Evidence Blocks Inject Cost into Doctor-Patient Talk
Author(s):
The NCCN announced a new series of cancer regimen guidelines that incorporate cost considerations to aid and facilitate broader discussion between physicians and patients about treatment.
Robert Carlson, MD
The National Comprehensive Cancer Network (NCCN) announced a new series of cancer regimen guidelines that incorporate cost considerations to aid and facilitate broader discussion between physicians and patients about treatment.
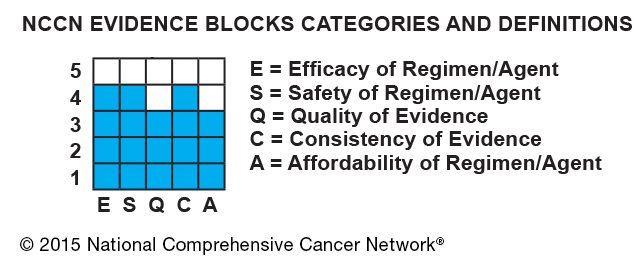
The NCCN, a nonprofit alliance of 26 cancer centers, said its Evidence Blocks combine efficacy, safety, quality of evidence, consistency of evidence, and affordability, and represent those variables simply in a matrix block that awards each of the criteria a score from 1 to 5, with a score of 1 being the lowest.
The first two sets of evidence blocks were released for treatment options for chronic myelogenous leukemia (CML) and multiple myeloma (MM), with as many as four more sets to be added by the end of this year, 10 next year, and the remainder — for all 61 NCCN guidelines – to be finished by the end of 2017.
Affordability of the regimens in the guidelines is based on a spectrum of cost considerations that include the overall treatment cost, toxicity, and other elements of care, and not just the cost of a particular drug, Robert Carlson, MD, CEO of the NCCN, said.
“We did not provide a dollar amount, because as soon as you do, your methodology requires that, and dollar amounts are virtually impossible to come by,” Carlson said in a press conference.
Carlson said variability of costs between treating institutions and also individual differences in patient condition and choices in care complicate the search for exact cost totals for particular regimens; however, he said there was very strong consistency in consensus estimates of cost among panelists who contributed to the matrix rankings compiled so far.
Even so, simply having an affordability ranking assigned to a particular regimen can constitute a valuable aid to a patient who is facing a huge amount of information and struggling not only to comprehend the treatment choices available but also to overcome the shock and confusion associated with the emotional blow of having a cancer diagnosis, said cancer patients who spoke in support of the Evidence Blocks at the press conference.
“The evidence block demystifies the discussion of cost,” added George Somlo, MD, of City of Hope Comprehensive Cancer Center of Duarte, California, a member of the NCCN Guidelines Panels for Breast Cancer and Multiple Myeloma. “Very few physicians are competent to talk about affordability,” he said.
A large proportion of personal bankruptcies have been shown to be the result of a medical expense pile-ups, and physicians are not sufficiently aware of the financial impact treatment decisions are having on their patients, Somlo said.
“My suspicion is that the physicians who were treating those patients had no clue what they were doing to those patients’ finances,” he said.


The Evidence Blocks are assigned to multiple possible regimens, and, further, regimens are divided into preferred and less-preferred columns. Somlo explained that comparative data and the amount and quality of evidence are key to which column a regimen appears in, with solid phase III evidence being a main determinant. This, he said, would explain why a hot new therapy with great potential would end up in the less-preferred column, as sufficient trial evidence had not been accumulated.
Ideally, patients and doctors would hold in-depth discussions about the multiple factors that go into individual treatment decisions, Carlson and Somlo said. Whereas cost might be a more important consideration for one patient than another, the risk of neuropathy might be a greater consideration to a professional pianist who relies on finger sensitivity, they said.
Breast cancer survivor Marta Nicols, who has become a patient advocate since her diagnosis 10 years ago, said the Evidence Blocks provide critical simplification of the process for patients who are facing “an entirely different language” when they are first exposed to the breadth of treatment options and medical terminology.
There’s much more pressure on the patient, given the wider variety of treatment options, to participate in selecting a course of therapy, she said.
“Today, it’s intended to be a collaborative process, where the physician is expecting the patient to make the decision,” Nicols, vice president of investor relations for GoDaddy, said.
The NCCN Evidence Blocks are but one of an increasing number of efforts lately to incorporate value into the treatment process. ASCO earlier this year came out with a rating system that it said was also in its prototype stages but that would be evolve into a means of assessing the value of new cancer therapies based on treatment benefits, toxicities, and costs.
In response to the NCCN announcement, ASCO Chief Medical Officer Richard L. Schilsky, MD, FACP, FASCO, said, “We believe that increasing efforts by different stakeholders in the cancer community to define value in cancer care further underscores the need for more transparency and information for patients and their doctors in making sound treatment decisions.


























