Publication
Article
Oncology Live®
CML Research Aims to Improve a "Magic Bullet"
Author(s):
The approval of imatinib almost 20 years ago heralded the arrival of the targeted therapy era in oncology and thrust the ABL1 kinase into the limelight.
Approval of imatinib (Gleevec) almost 20 years ago heralded the arrival of the targeted therapy era in oncology and thrust the ABL1 kinase into the limelight.1 A fusion involving the ABL1 gene is present in the vast majority of patients with chronic myeloid leukemia (CML), and aberrant ABL1 kinase activity is the central oncogenic driver in this cancer type.2
An inhibitor of the BCR-ABL1 protein, imatinib shaped a new standard of care for patients with CML. To address its limitations, including drug resistance, second and third generations of inhibitors have been developed. These agents have ultimately demonstrated superior efficacy to imatinib and expanded the frontline treatment arsenal for CML.3-5
Credited with transforming patients’ prognosis,6 BCR-ABL1 inhibitors do not yet offer a traditional “cure,” but they do promise long-term and, in some cases, potentially treatment-free disease control.7-9
The most recently approved BCR-ABL1 inhibitor, ponatinib (Iclusig), reflects efforts to specifically address the highly resistant BCR-ABL1 T315I mutation that drives resistance to all other BCR-ABL1 inhibitors.10
However, ponatinib is far from the final chapter; the story continues to evolve, with several new inhibitors in clinical development.
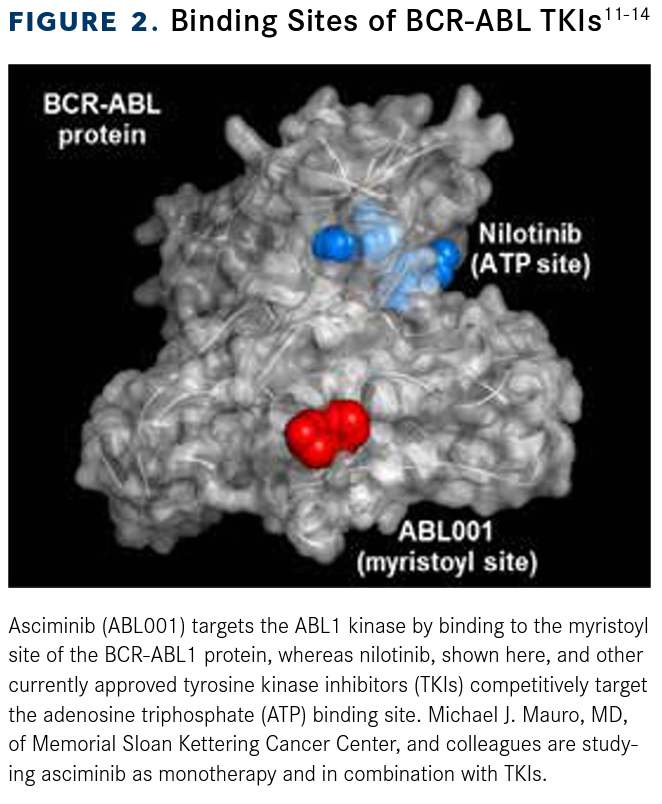
Novartis’ asciminib (ABL001) stands out for its novel mechanism of action; it is a first-in-class allosteric inhibitor that selectively targets ABL kinases.11 This mechanism contrasts with the currently approved agents, which inhibit BCR-ABL1 activity by competing with adenosine triphosphate (ATP) for binding to the ATP binding site on the kinase. Asciminib has demonstrated promise as both monotherapy and in combination with traditional inhibitors, indicating that the best may be yet to come in leukemia treatment.11-14
A Cancer Enabler
ABL1 and the highly homologous protein ABL2 (also known as ABL-related gene [ARG]) are nonreceptor tyrosine kinases (NRTKs)2, a subgroup of the tyrosine kinase enzyme family that lacks the receptorlike features of extracellular ligand-binding and transmembrane domains.15
NRTKs tend to be found in the cytoplasm, although they can be anchored to the membrane.15 ABL1 contains a DNA-binding domain, nuclear localization signal, and nuclear export signal, which allow it to localize to both the nucleus and the cytoplasm. ABL2 lacks these domains and is exclusively cytoplasmic.
Both proteins contain SRC homology domains (SH1, SH2, and SH3), an N-terminal cap region (which can be modif ied by myristoylation and plays a critical regulatory role in ABL kinase activity), F-actin—binding domains, and proline-rich sequences (the latter mediating interactions with other proteins).2,16
Click to Enlarge


The ABL1 gene was first described in 1970 as the normal cellular counterpart of a virally encoded gene found in a mouse leukemia virus that could transform normal mouse lymphocytes and fibroblasts. The viral protein was shown to have tyrosine kinase activity.16,17
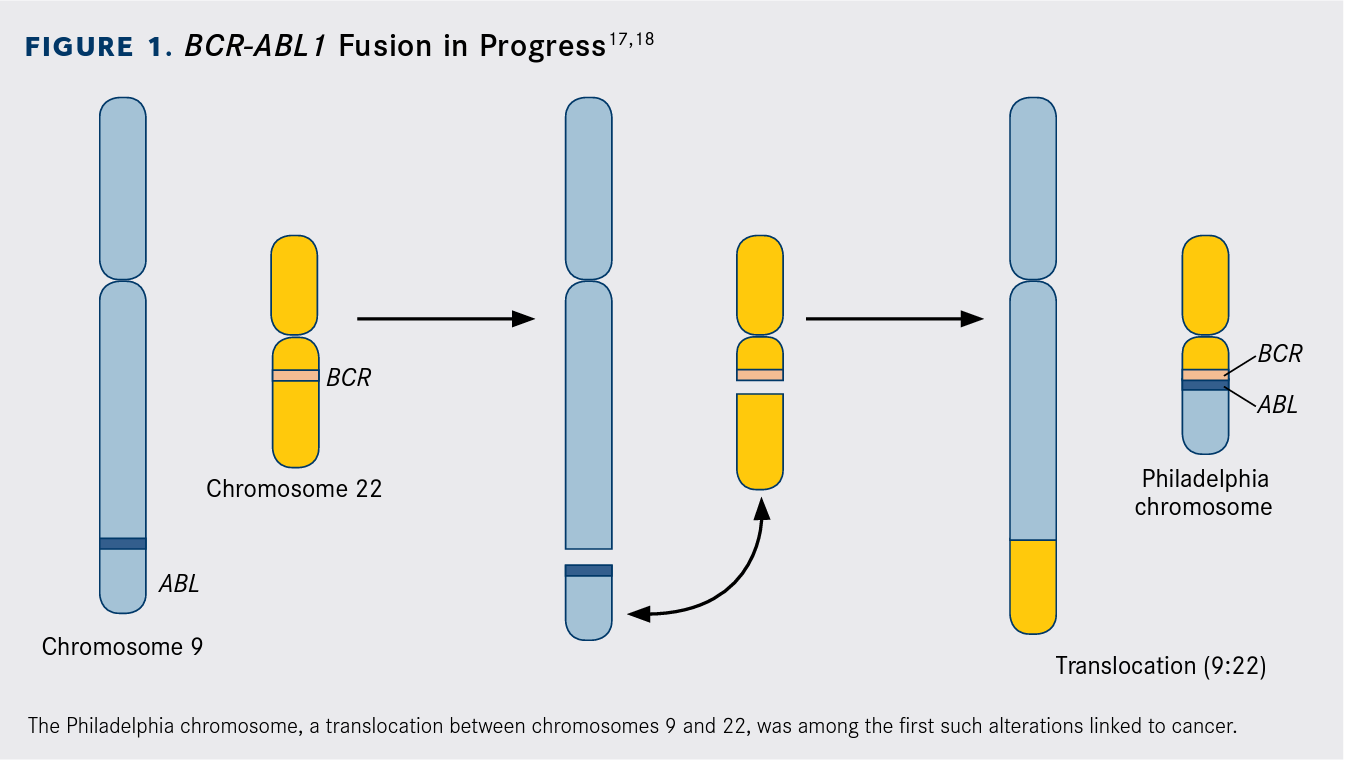
About 10 years earlier, investigators had discovered an unusual chromosome in the leukocytes of patients with CML, dubbed the Philadelphia chromosome after the city in which it was first described. Through a series of seminal studies, it was shown that the Philadelphia chromosome is the result of a chromosomal translocation involving chromosomes 22 and 9, the latter containing the human ABL1 gene (Figure 1).17,18
This chromosomal translocation generates a gene fusion, in which the ABL1 gene is fused in frame with a second gene known as breakpoint cluster region (BCR). The fusion results in constitutive activation of ABL1 kinase activity, which drives development of leukemia by promoting uncontrolled proliferation of undifferentiated immune precursor cells.4,17,18
Click to Enlarge


Oncogenic fusions involving both ABL1 and ABL2 have been identified in other forms of leukemia, such as T-cell ALL and acute myeloid leukemia, but have not been explored to the same degree.16,19 In the past decade, a potential role of ABL kinases in solid tumors also began to be appreciated. The mechanism of ABL activation is different in solid tumors; increased gene and protein expression and, more rarely, somatic mutations, rather than gene fusions, have been observed across a range of solid tumors, more commonly involving ABL2 than ABL1. 20
Poster Child for Precision Medicine
The significance of the BCR-ABL fusion in CML prompted a search for small molecules that could block its oncogenic kinase activity. Imatinib was the first tyrosine kinase inhibitor approved by the FDA for the treatment of cancer, earning it the cover of Time magazine, which described it as a “magic bullet.”21
Imatinib also inhibits c-KIT and platelet- derived growth factor receptor—α kinases. It was shown to be safe and effective across all phases of CML and was first approved for the treatment of Philadelphia chromosome–positive (Ph+) CML for patients resistant or intolerant to interferon alfa, the standard of care at the time.1 The following year, imatinib was approved for the treatment of all patients with newly diagnosed CML after it demonstrated superior efficacy in the phase III IRIS trial (NCT00006343).22
Later, imatinib was approved for patients with Ph+ ALL, in both the relapsed/refractory and frontline settings, with the latter in combination with chemotherapy and only in pediatric patients.23
Although the development of imatinib was undoubtedly a significant advancement, many patients are either intolerant or experience progression due to resistance. Numerous mechanisms of resistance have been uncovered, including those involving secondary BCR-ABL1 mutations that block imatinib binding or render it ineffective and those that are BCR-ABL1 independent, such as reduced drug uptake or increased drug efflux.4
The second-generation BCR-ABL1 inhibitors, dasatinib (Sprycel), nilotinib (Tasigna), and bosutinib (Bosulif), were designed to address these shortcomings. Like imatinib, they are ATP-competitive inhibitors, and each targets other kinases in addition to ABL, which leads to unique toxicity profiles.4,18
All 3 drugs were initially approved in the second-line setting after failure of imatinib and have subsequently been approved in patients with newly diagnosed CML following clinical trials demonstrating faster and deeper treatment responses, although none has been shown to improve overall survival (OS) to date.24-26
Although these drugs can successfully overcome many mechanisms of resistance to imatinib, they are all ineffective in the face of the so-called gatekeeper mutation, T315I, a single-amino acid change that alters the accessibility of the ATP-binding pocket of BCR-ABL.2 The only available third-generation drug, ponatinib, was designed to specifically inhibit this mutation and was approved for the treatment of patients with T315I-positive CML and ALL and for patients with these cancers for whom no other therapy is indicated.27
Ponatinib is currently approved only in the second-line setting in both disease indications. Clinical trials in patients with previously untreated CML demonstrated that its efficacy in this setting was limited by substantial toxicity.28 Ponatinib continues to be evaluated in the frontline setting in ALL, and recent results from a trial in which it was combined with hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (hyperCVAD) with alternating methotrexate and cytarabine demonstrated potential for long-term efficacy and safety.29
BCR-ABL inhibitors have revolutionized the treatment of CML, with 5-year survival rates now approaching the level of the general population.6 Although they do not offer a traditional “cure”—in virtually all patients with clinical disease remission, BCR-ABL transcripts are still detectable— BCR-ABL inhibitors can lead to deep and durable reduction of these transcripts, a so-called deep molecular response, which allows many patients to discontinue treatment and enjoy a “functional cure.”18
Click to Enlarge


Is the Best Yet to Come?
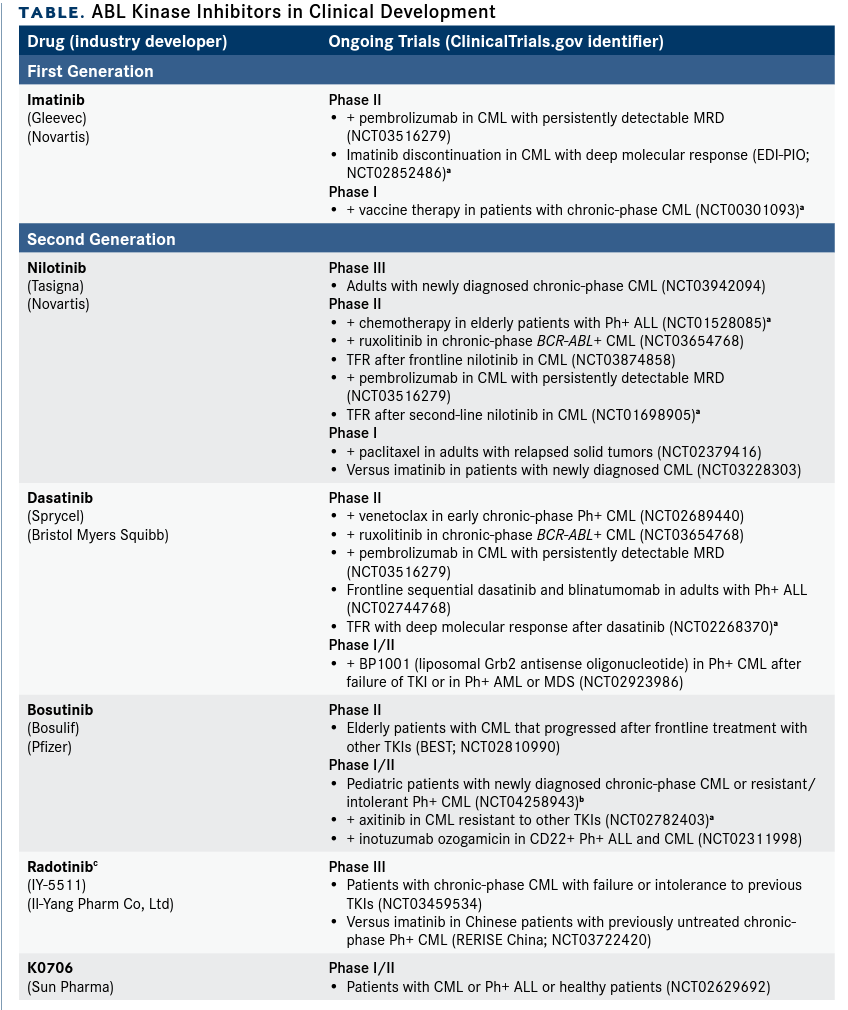
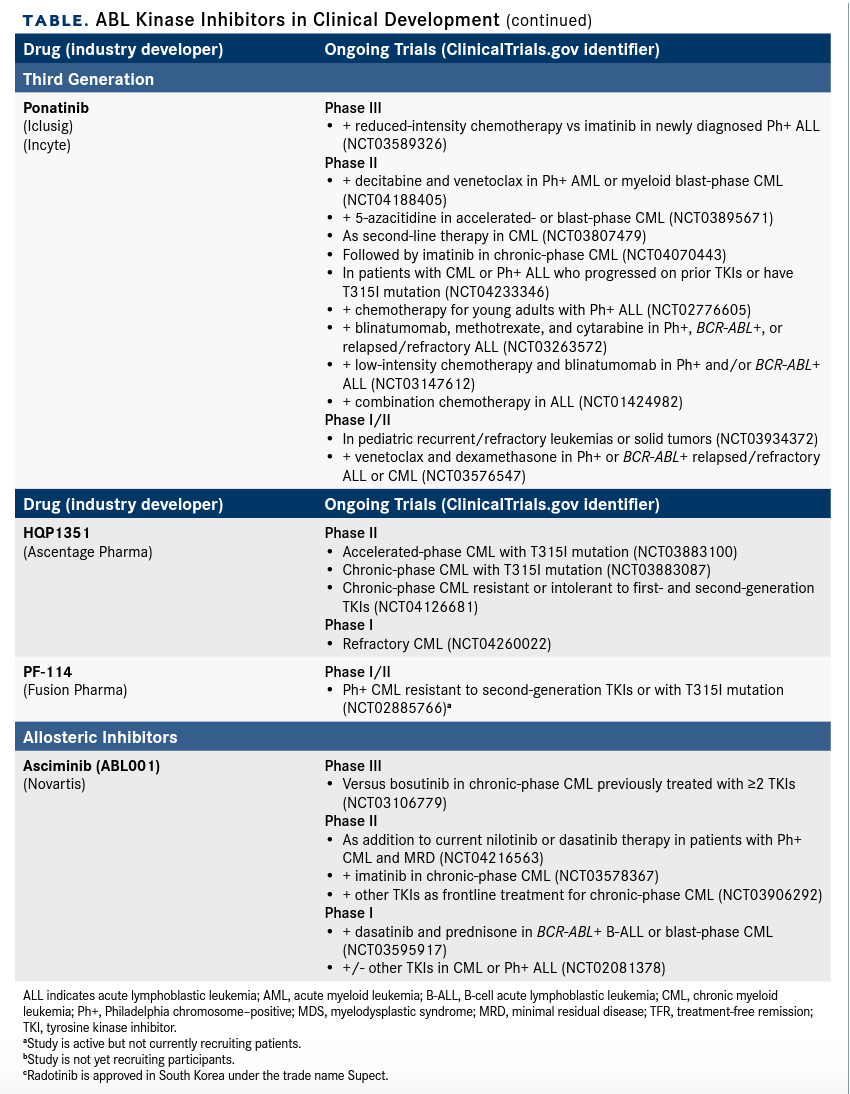
Meanwhile, the development of BCR-ABL inhibitors continues to evolve, with several newer drugs and combinations in clinical trials (Table). Most notable is asciminib, the first allosteric inhibitor of BCR-ABL1, which capitalizes on the autoinhibitory function of the N-terminal cap of the ABL1 protein.11
When myristoylated, that cap binds to a pocket in the kinase domain, serving as an allosteric negative regulator of ABL function. The cap (and thus the autoinhibition) is lost in the fusion protein; asciminib is designed to bind to the empty pocket and restore inhibition of BCR-ABL kinase activity (Figure 211-14). In contrast to the more promiscuous ATP-competitive inhibitors, asciminib is a highly specific inhibitor of ABL kinases. Critically, it is also effective against T315I-positive CML.11,18,31
The results of a phase I study of asci-minib in patients with CML were recently published (NCT02081378). A total of 150 patients with heavily pretreated disease were enrolled and treated with asciminib on either a once-daily schedule (n = 52) at doses of 80, 120, or 200 mg or a twice-daily schedule (n = 98) at doses of 10, 20, 40, 80, 150, 160, or 200 mg. Most of the participants (141; 94%) had chronic-phase CML, and 113 (80%) lacked the T315I mutation. Within this subset of 113 patients, 34 of 37 (92%) who did not have a complete hematologic response (CHR; defined as normalization of the complete blood count) at baseline achieved CHR during the study, and 31 of 57 patients (54%) without a complete cytogenetic response (CCyR; defined as the absence of Ph+ cells in the bone marrow) at baseline achieved CCyR in a median time of 24 weeks.
(Continued; Click to Enlarge)


Asciminib is also showing promise in combination with ATP-competitive inhibitors. Preliminary results from 34 patients enrolled in a phase I study (NCT02081378) evaluating the combination of asciminib with dasatinib or nilotinib in patients with CML resistant or intolerant to ≥2 prior BCR-ABL1 inhibitors were presented at the 24th Congress of the European Hematology Association (EHA 2019). Among patients who did not have BCR-ABL1 transcript levels <1% on the International Scale at baseline, 43% and 56% of patients in the nilotinib and dasatinib arms, respectively, achieved this by 48 weeks, and 31% and 36% of patients without MMR at baseline achieved MMR within this time frame.14
In a separate presentation at EHA 2019 (NCT02081378), the combination of asciminib and imatinib was also shown to be effective. Among the 25 heavily pretreated patients enrolled to date, the level of BCR-ABL1 transcripts was reduced to <1% in 60% of patients, to ≤0.1% (MMR) in 42%, and to ≤0.0032% in 15% by 48 weeks.
Asciminib combined with dasatinib and prednisone is also being tested in patients with newly diagnosed Ph+ ALL and CML, and results from the first 6 patients treated were detailed in a presentation at the 2019 American Society of Hematology (2019 ASH) Annual Meeting & Exposition (NCT03595917).13
Among other novel drugs are PF-114 and HQP1351, both ATP-competitive inhibitors designed to target the T315I mutation. An update on a phase I trial of HQP1351 in patients with treatment-resistant CML was presented at 2019 ASH. HQP1351 is admin-istered once every other day in 28-day cycles at doses ranging from 1 mg to 60 mg. Among 101 patients enrolled, over a median follow-up of 12.8 months, HQP1351 was well tolerated, except at the 60-mg dose. Among 68 patients without CHR at baseline, 92.6% achieved CHR, and 60.5% of the 95 patients without CCyR at baseline achieved that goal.32
K0706 and radotinib are novel second-generation inhibitors that inhibit common BCR-ABL1 mutations but not T315I. The latter is approved in South Korea, and the recent RERISE study (NCT01511289) found that it may yield similar long-term OS and progression-free survival and higher MMR rates compared with imatinib in patients with newly diagnosed CML, as well as lower rates of treatment failure and grade 3/4 neutropenia and hypophosphatemia.33
Jane de Lartigue, PhD, is a freelance medical writer and editor based in Gainesville, Florida.
References
- Cohen MH, Williams G, Johnson JR, et al. Approval summary for imatinib mesylate capsules in the treatment of chronic myelogenous leukemia. Clin Cancer Res. 2002;8(5):935-942.
- Tripathi R, Liu Z, Plattner R. EnABLing tumor growth and progression: recent progress in unraveling the functions of ABL kinases in solid tumor cells. Curr Pharmacol Rep. 2018;4(5):367-379. doi: 10.1007/s40495-018-0149-y.
- Kantarjian H, Shah NP, Hochhaus A, et al. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2010;362(24):2260-2270. doi: 10.1056/NEJMoa1002315.
- Rossari F, Minutolo F, Orciuolo E. Past, present, and future of Bcr-Abl inhibitors: from chemical development to clinical efficacy. J Hematol Oncol. 2018;11(1):84. doi: 10.1186/s13045-018-0624-2.
- Saglio G, Kim D-W, Issaragrisil S, et al; ENESTnd Investigators. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med. 2010;362(24):2251-2259. doi: 10.1056/NEJMoa0912614.
- Sasaki K, Strom SS, O'Brien S, et al. Relative survival in patients with chronic-phase chronic myeloid leukaemia in the tyrosine-kinase inhibitor era: analysis of patient data from six prospective clinical trials. Lancet Haematol. 2015;2(5):e186-e193. doi: 10.1016/S2352-3026(15)00048-4.
- Hughes TP, Ross DM. Moving treatment-free remission into mainstream clinical practice in CML. Blood. 2016;128(1):17-23. doi: 10.1182/blood-2016-01-694265.
- Saussele S, Richter J, Guilhot J, et al. Discontinuation of tyrosine kinase inhibitor therapy in chronic myeloid leukaemia (EURO-SKI): a prespecified interim analysis of a prospective, multicentre, non-randomised, trial. Lancet Oncol. 2018;19(6):747-757. doi: 10.1016/S1470-2045(18)30192-X.
- Saußele S, Richter J, Hochhaus A, Mahon FX. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30(8):1638-1647. doi: 10.1038/leu.2016.115.
- Cortes JE, Kantarjian H, Shah NP, et al. Ponatinib in refractory Philadelphia chromosome-positive leukemias. N Engl J Med. 2012;367(22):2075-2088. doi: 10.1056/NEJMoa1205127.
- Hughes TP, Mauro MJ, Cortes JE, et al. Asciminib in chronic myeloid leukemia after ABL kinase inhibitor failure. N Engl J Med. 2019;381(24):2315-2326. doi: 10.1056/NEJMoa1902328.
- Cortes JE, Lang F, Kim D, et al. Combination therapy using asciminib plus imatinib (IMA) in patients (PTS) with chronic myeloid leukemia (CML): results from a phase 1 study. Hemasphere. 2019;3(suppl 1; abstr S883):397. doi: 10.1097/01.HS9.0000561812.22500.d8.
- Luskin M, Murakami MA, Stevenson KE, et al. A phase I study of asciminib (ABL001) in combination with dasatinib and prednisone for untreated BCR-ABL1-positive ALL in older adults. Blood. 2019;134(suppl 1; abstr 3879). doi: 10.1182/blood-2019-125138.
- Mauro MJ, Kim D, Cortes JE, et al. Combination of asciminib plus nilotinib (NIL) or dasatinib (DAS) in patients (pts) with chronic myeloid leukemia (CML): results from a phase 1 study. Hemasphere. 2019;3(suppl 1; abstr S884):397-398. doi: 10.1097/01.HS9.0000561816.04574.8b.
- Neet K, Hunter T. Vertebrate non-receptor protein—tyrosine kinase families. Genes Cells. 1996;1(2):147-169. doi: 10.1046/j.1365-2443.1996.d01-234.x.
- Khatri A, Wang J, Pendergast AM. Multifunctional Abl kinases in health and disease. J Cell Sci. 2016;129(1):9-16. doi: 10.1242/jcs.175521.
- Rowley JD. Genetics. A story of swapped ends. Science. 2013;340(6139):1412-1413. doi: 10.1126/science.1241318.
- Soverini S, Mancini M, Bavaro L, Cavo M, Martinelli G. Chronic myeloid leukemia: the paradigm of targeting oncogenic tyrosine kinase signaling and counteracting resistance for successful cancer therapy. Mol Cancer. 2018;17(1):49. doi: 10.1186/s12943-018-0780-6.
- Greuber EK, Smith-Pearson P, Wang J, Pendergast AM. Role of ABL family kinases in cancer: from leukaemia to solid tumours. Nat Rev Cancer. 2013;13(8):559-571. doi: 10.1038/nrc3563.
- Wang J, Pendergast AM. The emerging role of ABL kinases in solid tumors. Trends Cancer. 2015;1(2):110-123. doi: 10.1016/j.trecan.2015.07.004.
- Lemonick MD, Park A. New hope for cancer. Time. May 28, 2001. content.time.com/time/world/article/0,8599,2047900,00.html. Accessed March 10, 2020.
- O'Brien SG, Guilhot F, Larson RA, et al; IRIS Investigators. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2003;348(11):994-1004. doi: 10.1056/NEJMoa022457.
- Gleevec [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2018. www.accessdata.fda.gov/drugsatfda_docs/label/2018/021588s053lbl.pdf. Accessed March 10, 2020.
- Sprycel [package insert]. Princeton, NJ: Bristol-Myers Squibb Company; 2018. www.accessdata.fda.gov/drugsatfda_docs/label/2018/021986s021lbl.pdf. Accessed March 10, 2020.
- Tasigna [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2019. www.accessdata.fda.gov/drugsatfda_docs/label/2019/022068s031lbl.pdf. Accessed March 10, 2020.
- Bosulif [package insert]. New York, NY: Pfizer Labs; 2019. www.accessdata.fda.gov/drugsatfda_docs/label/2019/203341s017lbl.pdf. Accessed March 10, 2020.
- Iclusig [package insert]. Cambridge, MA: Takeda Pharmaceutical Company Limited; 2020. www.accessdata.fda.gov/drugsatfda_docs/label/2020/203469s031lbl.pdf. Accessed March 10, 2020.
- Jain P, Kantarjian H, Jabbour E, et al. Ponatinib as first-line treatment for patients with chronic myeloid leukaemia in chronic phase: a phase 2 study. Lancet Haematol. 2015;2(9):e376-e383. doi: 10.1016/S2352-3026(15)00127-1.
- Short NJ, Kantarjian HM, Ravandi F, et al. Long-term safety and efficacy of hyper-CVAD plus ponatinib as frontline therapy for adults with Philadelphia chromosome-positive acute lymphoblastic leukemia. Blood. 2019;134(suppl 1; abstr 283). doi: 10.1182/blood-2019-125146.
- National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology. Chronic Myeloid Leukemia (version 3.2020). nccn.org/professionals/physician_gls/pdf/cml.pdf. Accessed March 10, 2020.
- Zhang J, Adrián FJ, Jahnke W, et al. Targeting Bcr-Abl by combining allosteric with ATP-binding-site inhibitors. Nature. 2010;463(7280):501-506. doi: 10.1038/nature08675.
- Jiang Q, Huang X, Chen Z, et al. An updated safety and efficacy results of phase 1 study of HQP1351, a novel 3rd generation of BCR-ABL tyrosine kinase inhibitor (TKI), in patients with TKI resistant chronic myeloid leukemia. Blood. 2019;134(suppl 1; abstr 493). doi: 10.1182/blood-2019-124295.
- Do YR, Kwak J-Y, Kim JA, et al. Long-term data from a phase 3 study of radotinib versus imatinib in patients with newly diagnosed, chronic myeloid leukaemia in the chronic phase (RERISE) [published online February 3, 2020]. Br J Haematol. doi: 10.1111/bjh.16381.
A major molecular response (MMR; defined as BCR-ABL1 transcript levels ≤0.1% on the International Scale) was achieved or maintained by 12 months in 48% of evalu-able patients in this subset, including 57% with resistance to or intolerable toxicity from ponatinib. In contrast, 28% of patients with chronic-phase CML who had the T315I mutation achieved or maintained MMR by 12 months.11
It was initially thought that only lifelong treatment could maintain functional cure, but several studies demonstrated that certain patients with a deep molecular response can stop long-term BCR-ABL inhibitor therapy without relapsing for significant periods of time.18 The European Stop Kinase Inhibitor trial, for example, demonstrated treatment-free remission for approximately half of patients being treated with any of the frontline BCR-ABL inhibitors.8 Numerous ongoing studies are examining this phenomenon, and the latest guidelines from the National Comprehensive Cancer Network suggest that stopping treatment with close monitoring is feasible in carefully selected patients.30
The Philadelphia chromosome has been shown to be present in leukemia cells in more than 95% of CML cases and has been identified in a significant proportion of patients with acute lymphoblastic leukemia (ALL). The specific transcript involved in B-cell ALL is slightly different as a result of different breakpoints within the BCR gene, and it encodes a lower-molecular-weight protein referred to as p190BCR-ABL1; in CML, it is p210BCR-ABL1.18
In normal cells, the ABL kinases are activated by a wide range of stimuli and function in diverse cellular processes, including many of the hallmarks of cancer, such as proliferation and migration, in addition to cytoskeletal reorganization, adhesion, and beyond.16