

|Videos|January 29, 2021
Optimizing First-Line Therapy in mCRC
Axel Grothey, MD, and John Marshall, MD, discuss strategies for optimizing first-line treatment in metastatic colorectal cancer and the role of adjuvant therapy.
Advertisement
Episodes in this series
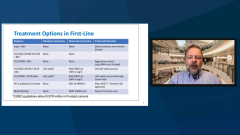







John Marshall, MD: What’s our first and best chance at a response induction therapy? It’s where we get our highest response rates. They are most durable for almost all the sequence that they’re about to head off on. And the old tradition, of course, was to give this for a magical 12 cycles for 6 months. And it was almost a bravado among physicians that they felt obligated to get to that 12 cycles, or that 6 months, as though it was some rule, as though it was the law.
And I know we see eye to eye on this. For me, I tell a patient right from the beginning when we’re setting out on induction, “We’re going to take a look at about 3 months. And if you’ve had a nice response, I’m not going to go much longer because I’m not going to get much more response. But I’m going to take those drugs that got us there back off the table and try to. Instead of how much chemotherapy can I give you, it now switches…to how little chemotherapy I’m going to give you, assuming that we have a noncurative approach. How do you handle that? Are you taking people to 6 cycles or 6 months, or are you stopping on your maintenance a bit earlier?
Axel Grothey, MD: First of all, there’s really no magic to 6 months or 12 cycles or whatever you might call it; there’s absolutely none and I actually educate my patients right up front about this induction maintenance therapy or when I plan a change in treatment intensity. Because I don’t want them to say, “Oh my God, what’s happening” when we’re changing treatment. They need to know about this. And when you educate them about this up front, when you provide the rational, you know the initial response is the strongest. You do a first scan after 4 cycles, 2 months, let’s say 6 months, 6 cycles, 3 months, whatever you like. I do it after 2 months.
You see the stronger response then when you did the next scan. Your initial response is stronger. And then eventually you maintain the response. I tell my patients I want to turn this into chronic disease; again, using the least amount of treatment necessary to control it. And I tell them, all right, especially when you start the FOLFOX [fluorouracil oxaliplatin]-based therapy, you’re obligated to stop oxaliplatin before patients run into issues.
With irinotecan-based therapy, if you’re a FOLFIRI fan, you know first line, there’s nothing wrong with that, I still do de-escalation. Probably not as rigidly after 8 cycles, because you can push past, you live longer, but you don’t have to.
I strongly believe that at some point the tumor cells that are…still around are resistant to the intense treatment. Then it’s really kind of using capecitabine [CAPE]-BEV [bevacizumab]. I know you and I see on that eye to eye, too, as maintenance therapy and to try to maintain quality of life.
John Marshall, MD: Yes. We can’t forget that we want that patient’s bone marrow and liver function to be good maybe 2 years from then, right?
Axel Grothey, MD: Yes.
John Marshall, MD: If they’re doing well and if we keep giving them chemotherapy cycle after cycle, we’ll wear them out physically and also wear out the nonrenewable, unlimited resources of bone marrow and liver. I do the same if it’s with irinotecan. And, it’s even become more interesting in the triplet front line because then I’m pulling these other drugs back and…I sort of describe it as a chest game. I haven’t lost a piece, they’ve just moved it; leave it on the board there for a while and we’re going to move it again later. But if we can get by with a few pawns for a while, what a great way to go. And I’m the same way with the CAPE-BEV.
Axel Grothey, MD: One thing I get asked, when you start with a triplet, which I do more and more, what do you do in second line? I say, this is not the question because second line happens on maintenance or in treatment-free interval. The median progression-free survival of these triplet combinations is 12 months plus. However, patients still get treated for 12 months with a triplet. We stop treatment after 4 or 6 months and then when they progress you can reinitiate. And you use oxaliplatin, irinotecan, whatever, again.
John Marshall, MD: I almost never totally stop chemotherapy when people have visible metastatic disease. There are a few exceptions. For instance, when patients with very small volume disease that’s already proven itself to be very quiet, I’ll take 3 months off, something similar to that.
I did that this past summer. I gave a young man with metastatic disease the summer off, partly because of COVID-19 [coronavirus disease 2019], and, yes, he progressed, but not very much. We didn’t lose much ground in 3 months.
Axel Grothey, MD: I do that, too, maybe try to see around special days, vacation, holidays, family events, whatever. But 1 issue is we need to keep a close eye on these patients, and we need to know tumor biology. And there’s a point when you go to maintenance, you already know tumor biology of this patient. And not every patient is the same. My default is to keep patients on some form of treatment.
John Marshall, MD: I’m the same way. And this is a little special scenario of the patient who is fortunate enough to have retractable disease. Just as a quick little aside before we move into beyond progression, if you will.
There are data now that adjuvant therapy really doesn’t do its adjuvant thing. It might delay relapse, but it didn’t cure more people. The 3 months of adjuvant therapy, now the norm, it sort of made me change my thinking if I was giving induction chemotherapy, neoadjuvant, for example, and now we resect metastasectomy. I’m probably doing a ctDNA [circulating tumor DNA] test afterward to see if it’s negative. But then I’m probably leaving him alone more and more. What do you think?
Axel Grothey, MD: You know, you brought up an interesting point. As you were talking, I was thinking this is exactly where we need to have ctDNA.
Because there are some patients who don’t benefit from adjuvant therapy who have recurrence anyway, and there are some patients who don’t need it, they will not have a recurrence. We’re overestimating the importance of postoperative adjuvant therapy once you’ve given neoadjuvant treatment, which we commonly do in the metastasectomy setting. Because we can see the response, see the chemosensitivity. Regarding ctDNA, the minimal residual disease, there are trials that are being run right now that will completely change the way we use adjuvant therapy. It’s adjuvant therapy when you need it, when you start turning positive and then you can spare adjuvant treatment for a lot of patients.
John Marshall, MD: I still get questions almost once or twice a week from our community partners asking, “Can’t I give 6 months of adjuvant therapy?” I say, “You’re done, you’re okay, it’s fine.” It’s been so hard for people to let go of those additional 3 months. I don’t know if you’re getting the same sort of feedback.
Axel Grothey, MD: It’s still interesting, and some of these trials are still using 6 months as a default. You know, as a control arm, and that’s hard to justify because…if you really talk about 6 months of adjuvant FOLFOX-based therapy, that’s a lot of toxicity, persistent toxicity.
John Marshall, MD: Yes, it’s too much.
Transcript Edited for Clarity
Advertisement
Related Content




Latest CME































Advertisement
Advertisement
Trending on OncLive
1
Long-Term Cilta-Cel Data Show Low Rates of PFS Events in Standard-Risk R/R Myeloma
2
Real-World Data Support Clinical Benefit With Lifileucel in Previously Treated Advanced Melanoma
3
FDA Updates Axi-Cel Label to Remove Limitation of Use in R/R PCNSL
4
Dr Riedell on the Long-Term Efficacy of Tisa-Cel in R/R Follicular Lymphoma
5