Now Playing

Your AI-Trained Oncology Knowledge Connection!
Axel Grothey, MD, discusses factors that influence treatment selection in patients with mCRC.
John Marshall, MD: Good evening, everybody. My name is Dr John Marshall and joining me tonight is my good friend and colleague, and really the world’s expert on gastrointestinal cancers and colorectal cancer, Dr Axel Grothey.
We want to welcome everybody to an OncLive® event. Our focus tonight is on the management of metastatic colorectal cancer [mCRC]. And as I mentioned, I am John Marshall from Georgetown University, director of the Ruesch Center for the Cure of Gastrointestinal Cancers. And Axel, of course, is known to everybody. He is the director of Gastrointestinal Cancer Research at the West Cancer Center & Research Institute in Germantown, Tennessee.
Axel and I are going to talk about the optimum treatment for metastatic colorectal cancer [mCRC]. And there are a lot of new data that you need to be aware of. We will remind you of some important older data as we talk about clinical scenarios through lines of therapy, including what is the right first-line therapy.
We’re going to talk about maintenance therapy and how best to optimize chemotherapy lite or chemotherapy free interval. And then we’re going to talk about later lines of therapy, second, third, and beyond.
Axel, it seems we went from a time of 5FU [fluorouracil] only, then FOLFOX [folinic acid, fluorouracil, and oxaliplatin] for everybody. And now with molecular profiling, it’s not a straightforward 1-size-fits all front line for everybody. Give us your sense of how you figure out that new patient in front of you with metastatic disease. What are you going to do with him? What are you going to give? What molecular testing do you need to know, etc?
Axel Grothey, MD: It’s not a 1-size-fits-all front line. I still believe that in the United States most patients will receive FOLFOX plus bevacizumab as their “go-to.” It’s the broad-spectrum antibiotics that we use when we don’t know what to do or which bug we are actually treating.
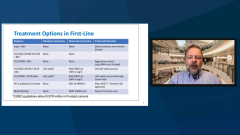
And this is for a good reason. FOLFOX plus bevacizumab has activity in left- and right-sided tumors independent of the molecular profile that we have, but we can do better. And this slide here that you highlighted just now looked at what I like to present as the factors influencing treatment choices in metastatic colorectal cancer. Of course, these are patient characteristics. We’re treating older patients differently than younger patients. This is not ageism; it’s just about how patients tolerate things. And we have some patients who have been pretreated with adjuvant therapy. Performance status is a big issue.
The goal of therapy is patient preference, but more and more it will be the molecular characteristics. And the 4 factors that you see on the right upper side, the RAS mutation analysis, BRAF mutation, and HER2, are the cornerstones of what we really need. It is kind of the basis of molecular testing that can really guide therapy.
I would even include the tumor location as 1 of the factors that has similar standing as the molecular factors to the idea that tumor location, right-sided tumors, meaning anything proximal to the hepatic and splenic flexure, based on some European data, those tumors do not respond to EGF receptor antibodies when added to chemotherapy. And data are consistent that those tumors, even when they’re RAS wild type, BRAF wild type, do not respond to cetuximab or panitumumab. It is tumor location as a predictive factor. And it’s also a prognostic factor; right-sided tumors do worse than left-sided tumors. That is really kind of setting the stage for our treatment decision.
Transcript Edited for Clarity