

|Videos|February 4, 2021
Using Molecular Testing to Guide Treatment Selection in mCRC
John Marshall, MD, and Axel Grothey, MD, discuss how molecular testing results guide treatment decisions in patients with mCRC.
Advertisement
Episodes in this series







John Marshall, MD: It’s funny. When I send off molecular profiling, and I receive the result back, I click on the website, and there’s almost an excitement when I get 1 of these positive markers. Now, a BRAF of course is bad news, but at least I have more to do about that for a V600E patient.
When I receive MSI [microsatellite instability], I almost close my eyes and look again and think, “Do we have the right result?” I never believe the IHC [immunohistochemistry]. I always repeat the genetics just to make sure. And tumor mutational burden [TMB] has become a last-line salvage. If I did a test 2 years ago and the TMB was 12, I’m in, because now got approval. HER2 [human epidermal growth factor receptor 2], for me at least, has been rare. I look in almost everybody, and it’s rare that I have a HER2+ colon. And I see a ton of patients with colon cancer.
Axel Grothey, MD: I agree.
John Marshall, MD: Whenever I get 1 of these, I get a little excited. Then I think, “Do I go ahead and use it now? Do I stop what I’m doing? Let me pick on some of the easy ones, like MSI high. Is it first line for everybody? What if I’ve got a patient with a big tumor burden who is symptomatic?
Axel Grothey, MD: It’s hard to make a case against I/O [immuno-oncology] therapy in first line. The data are convincing, and we should embrace that. We have randomized data now. It’s a good reason to do this and not wait too much longer. But there is 1 caveat. The KEYNOTE study has this higher rate of early progressors: 29.4% compared 12.6%. And the switch, the crossover of the PFS [progression-free survival] data—I would love to know who those patients are. The publication is pretty meager on exactly that.
John Marshall, MD: Incredibly meager.
Axel Grothey, MD: I would like to see TMB analysis. What kind of mismatch repair proteins were deactivated? There’s tons of analysis that we can do and hopefully will be done. We can potentially even look at patients who need combination with chemotherapy in lung cancer. If you have lung cancer expressing less PD-L1, non–small cell lung cancer, you combine with chemotherapy because you want a response. Because the benefit is if you have a response. In the KEYNOTE study, 83% of patients who have a response will continue to have a response after 2 years.
That’s the excitement I have. We can cure patients with stage IV disease with immunotherapy when they’re MSI high. Those are loaded words, you know?
John Marshall, MD: I’ve got some who obviously haven’t been. But there will be some.
Axel Grothey, MD: There will be some.
John Marshall, MD: I hope that’s right. I keep coming back to the point—maybe it’s the same 1 you’re making—that never before have we had a biomarker in MSI where it’s not very clearly written how that has to be tested. You can use immunohistochemistry, with 1 of 4 proteins missing, even though we know they’re not all the same. You can have DNA fragment analysis. You can do next-generation sequencing with computer analysis. At least from an FDA perspective, or equation, we’ll learn the marker may not be the same in all those people.
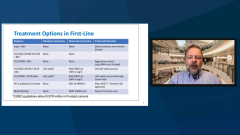
So MSI early on. BRAF? To me it’s still a second-line therapy. These are usually bad tumors. If I thought ahead, use FOLFOXIRI [5-fluorouracil, leucovorin, oxaliplatin, irinotecan] in the front line. If I get a maintenance window, I feel lucky. Then it’s a BRAF-targeting therapy second line. Is that where you are too?
Axel Grothey, MD: Agreed. We had data from a little bit more than 40 patients in the first line, and the ANCHOR-CRC study, which looked at the BEACON CRC triplet [encorafenib, binimetinib, cetuximab]. And there was a high response rate, 50%. Almost every patient had some form of tumor shrinkage. But the progression-free survival was 12.9 months. That’s not great, and that’s something I see even in a second- or third-line setting.
Once tumors have figured out how to counteract the BRAF-EGF receptor antibody inhibition of the MAP kinase pathway, they progress quite rapidly. I see this rapid emergence of resistance. That is something we need to work on: MET amplification, the EGF receptor amplification.
There are a lot of mechanisms that we pick up right now. We need to figure out what’s going to individualize even the treatment against the resistant clones over time.
John Marshall, MD: Right now, you’ve got tumor mutational burden of 13, OK? Let’s say you’ve had first- and second-line therapy, and I’m adding pembrolizumab into your choices. Now you have 4 drugs, right? Are you going to fight an I/O card with the TMB data, or are you going to use anEGFR inhibitor? What are you going to do?
Axel Grothey, MD: I’m a little skeptical about the cutoff of 10 for all tumors.
John Marshall, MD: Me too.
Axel Grothey, MD: I completely agree. I believe there’s a difference, which I see with a TMB of 10 or 20—with 20 I would have no problem using pembrolizumab earlier. Probably not in the first line. Potentially in the second-line setting, depending on patients’ preference and how they are. But in the third-line therapy study, those patients do benefit. They have a high chance of benefit.
Transcript Edited for Clarity
Advertisement
Related Content




Latest CME































Advertisement
Advertisement
Trending on OncLive
1
Single-Center, Retrospective Data Show Low Rate of Lifileucel Infusion Following Referral in Advanced Melanoma
2
Long-Term Cilta-Cel Data Show Low Rates of PFS Events in Standard-Risk R/R Myeloma
3
Real-World Data Support Clinical Benefit With Lifileucel in Previously Treated Advanced Melanoma
4
Dr Riedell on the Long-Term Efficacy of Tisa-Cel in R/R Follicular Lymphoma
5