

|Videos|August 9, 2021
Case 1: 75-Year-Old Man With SM
Dan DeAngelo, MD, PhD, presents the case of a 75-year-old man with systemic mastocytosis and reviews WHO diagnostic criteria.
Advertisement
Episodes in this series






Dan DeAngelo, MD, PhD: I’d like to go through some cases. These are real cases. These are cases I just pulled out from patients I’ve seen. This is a 75-year old gentleman. He had a 3-month history of abdominal distension and some lower-extremity edema. His blood counts, when he was finally referred in, showed a white blood cell count of 27,000 per mm3 with a hemoglobin of 8 g/dL and a platelet count of 64,000 per mm3. His differential was rather bland, with the exception that he had a nucleated red [blood] cell, no immature cells. The CT scan—I’ll show you a picture in a second—showed diffused lymphadenopathy about 2 to 3 cm, so pathologic lymphadenopathy. He had both small pleural effusion and ascites. The ascites was symptomatic, and he had splenomegaly. Of course, what was the next step? I checked the tryptase level and a bone marrow exam, because I’m a hematologist, so you use the tools in your toolbox. Also, with bone marrow examination, which I’ll show in a second, it showed the hypercellular marrow with 40% mast cells, and they were classic. We’ll have our pathologists comment on it in a second. CD117, and they had aberrant CD2 and CD25. Cytogenetics were normal, but he had a next-generation sequencing [NGS] panel that we call rapid heme panel that showed mutations in KIT, SRSF2, TET2, and COX1.
I hope that you can see the screen, but he had both hepatomegaly and splenomegaly. On this view, you can see some ascites around the liver and the spleen. But there was some more ascites, to the point that he had at least grade 2 ascites requiring diuretic therapy. Also, these are bone marrow exams from this particular patient. Highlighting the hypercellularity of the marrow, this is a low-power view, but with the spindle-shaped cells that were associated with some underlying fibrosis, it’s hard to differentiate what’s going on. The immunohistochemical stains in the bottom with a mast cell tryptase and a CD25 just to show aberrant. I’m not showing CD117 for brevity, but this highlighted the fact that this patient had a substantial population of aberrant mast cells making the diagnosis of systemic mastocytosis. The question, of course, is what subtype. He was at such a hypercellular marrow, it was hard to get an aspirate out of him, which shouldn’t surprise you. This is our next-generation sequencing platform.
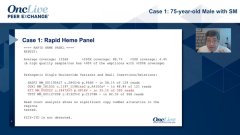
Highlighted in red is the characteristic pathognomonic KIT mutation that’s present in about 90% to 95% of patients. This gentleman had a pretty high allele burden, but he also had other mutations, such as a mutation in the spliceosome, a mutation in a DNA transfer TET2 and COX1. This is most consistent, especially giving this person leukocytosis of a subtype of systemic mastocytosis with an associated hematologic neoplasm. Just to take you through this—I’ll pass the baton to Dr Wang in a second—these are the WHO [World Health Organization] criteria for diagnosis. You have to have 1 major and 1 minor or 3 minor criteria. The major criterion is multifocal dense infiltrates of mast cells. I don’t think there’s any question that this person had these huge, dense infiltrates. An infiltrate is defined as an aggregate of 15 cells or more. The minor criteria are 4-fold. One is that a quarter of the cells have to have an atypical spindle cell morphology, which is really hard to see on the photos I showed. There has to be a KIT mutation, and I showed that. There has to be a CD25, which is aberrantly expressed. CD2 is another aberrant marker. This patient had CD25, so that’s a second minor. Then, a tryptase level of 20 ng/mL. This man’s tryptase was in the 100s approaching 200 ng/mL. Consequently, he clearly met 1 major and 3 minor criteria. Any way you slice or dice it, this patient met the diagnosis of systemic mastocytosis.
To highlight what we’ve talked about, this example was not difficult because the majority of the clone, the allele burden, was 35%, which means 70% of his disease was driven by KIT. But it can be very difficult, and Dr Bose had mentioned 1 of his cases. This shows the difference between NGS and the sensitivity of digital droplet PCR [polymerase chain reaction], which can really detect 1 or 2 cells out of a million. As a result, you can pick up about a third of cases with standard NGS, but in digital droplet PCR, you can pick up almost all the cases because almost 95% of cases will have a KIT mutation. This is a very important thing to remember. I get referred a lot of patients, and it would be interesting—after I present this case—to hear what Dr Bose’s thoughts are, on KIT wild-type systemic mastocytosis. But they did a nonsensitive NGS panel, sometimes at a place I’ve never heard of. When we repeat it with our digital droplet PCR, we’re often able to pick up a KIT mutation. This is very important to mention.
Transcript Edited for Clarity
Advertisement
Related Content





Latest CME































Advertisement
Advertisement
Trending on OncLive
1
Long-Term Cilta-Cel Data Show Low Rates of PFS Events in Standard-Risk R/R Myeloma
2
FDA Updates Axi-Cel Label to Remove Limitation of Use in R/R PCNSL
3
Real-World Data Support Clinical Benefit With Lifileucel in Previously Treated Advanced Melanoma
4
Nonresponse to Bridging Therapy and Peak ALC After Cilta-Cel Are Associated With Neurotoxicity, NRM in Myeloma
5