

|Videos|August 16, 2021
Case 1: Treatment and Management Considerations
The panel of experts in SM discuss the diagnosis and management of a 75-year-old man with systemic mastocytosis.
Advertisement
Episodes in this series

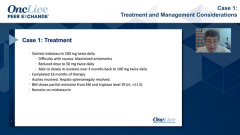





Dan DeAngelo, MD, PhD: This is very important to mention. This particular man went on to receive midostaurin. Midostaurin is the FDA-approved agent. Avapritinib, which we’ll talk about with the next case, was just approved. But Midostaurin is approved at a dosage of 100 mg twice daily, which is different from the dose that’s approved in AML [acute myeloid leukemia]. It’s not surprising that this man had some difficulty with nausea. I tried maximizing his antiemetics. I had to reduce the dosage to 50 mg twice daily. Over several months, he was able to tolerate the reduced dosage and antiemetic regimen, and I was able to scale his dosage back to 100 mg twice daily, which I always try. My experience has suggested that patients have a dose-response curve, so I try to get as much drug as I can. After a year and a half of therapy, he had a complete remission with resolution of his ascites, resolution of his hepatosplenomegaly, resolution of his bone marrow infiltrate, and a tryptase that was below 20 ng/mL, at 19 ng/mL. Still elevated but less than 20 ng/mL, and that’s the criterion for remission. He was still doing well on midostaurin. Prithviraj, what are your thoughts on the diagnosis and management?
Prithviraj Bose, MD: As you said, this is a very clear-cut case of SM [systemic mastocytosis] meeting multiple criteria. A lot of C findings as well. I noticed ascites. I saw hypersplenism with the low counts and the big spleen and then the 40% infiltrate in the marrow could have also been contributing to the cytopenias. In fact, I meant to ask you, did the cytopenias improve on the midostaurin?
Dan DeAngelo, MD, PhD: Yes, this is 1 of those unusual cases where the cytopenias—in my opinion, they don’t usually improve—in this case did improve because remember he had a leukocytosis that was probably being driven by this clone. Consequently, that was a peripheral blood NGS [next-generation sequencing] panel and his thrombocytopenia was likely because of his hypersplenism. Thus, when the spleen normalized, his platelets improved.
Prithviraj Bose, MD: Right. Going back to your point about the NGS missing the mutation, we too had a number of cases before we started doing the digital droplet PCR [polymerase chain reaction], where we were finding them to be KIT wild type. We’ve gone back and started to reflexively order the digital droplet PCR, or the molecular diagnostics people do, if they find the NGS is negative.
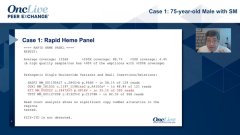
Dan DeAngelo, MD, PhD: That’s a great point. For any patient referred to us, specifically from our allergy colleagues, just because of the referral pattern much of the time, the patient is going to have a lower volume of disease. We’re dealing with mostly indolent systemic mastocytosis, because if they had C findings, they had often come in referred into a different mechanism. One of the checkboxes is that everybody gets a digital droplet PCR. Dr Wang, 1 of the highlights of this case is that this is not just systemic mastocytosis. This man has these 2 processes. He has some myeloproliferative stuff. He presented with a white blood cell count of 27,000 per mm3 and lots of mutations. How difficult can it be, and how do you make a diagnosis of SM-AHN [systemic mastocytosis with an associated hematologic neoplasm]?
Sa Wang, MD: We always like to discuss this among our own pathologists. Usually a patient with indolent SM, the CBC [complete blood count] is almost always normal. When you have significant cytopenia or cytosis, that’s the time you have to look for the underlying disease. Of course, they can be because of the C findings but also the underlying…malignancy. Another thing I’d like to point out is that the pathology I saw was quite interesting. I don’t know if you see patients with mast cell SM, but the bone always has a lot of changes. You can see those on the modeling. That probably corresponds to what you see on MRI [magnetic resonance imaging]. The bone always has a lot of bone changes.
Dan DeAngelo, MD, PhD: You mean the osteoclast?
Sa Wang, MD: This osteoclast and osteoblast is modular. They become thickened. It’s a very common thing in patients with systemic mastocytosis.
Dan DeAngelo, MD, PhD:I didn’t appreciate that. Thank you.
Sa Wang, MD: Another thing for the markers—we like to use CD1 c-KIT, CD117, because the tryptase a lot of times, especially when the mast cells become immature or aberrant, can lose tryptase. Tryptase a lot of times is more variable than the CD117. The CD117 usually highlights most of the mast cells.
Dan DeAngelo, MD, PhD: This patient did have a CD117, but I could put only 4.
Transcript Edited for Clarity
Advertisement
Related Content
Advertisement





Latest CME































Advertisement
Advertisement
Trending on OncLive
1
Single-Center, Retrospective Data Show Low Rate of Lifileucel Infusion Following Referral in Advanced Melanoma
2
Long-Term Cilta-Cel Data Show Low Rates of PFS Events in Standard-Risk R/R Myeloma
3
Real-World Data Support Clinical Benefit With Lifileucel in Previously Treated Advanced Melanoma
4
Dr Riedell on the Long-Term Efficacy of Tisa-Cel in R/R Follicular Lymphoma
5