

|Videos|September 13, 2021
Case 4: A 68-Year-Old Female With Mast Cell Leukemia
Sa Wang, MD, presents the case of a 68-year-old female with mast cell leukemia.
Advertisement
Episodes in this series






Sa Wang, MD: I’ll show a couple of cases. I don’t have very detailed treatment information, but I think I have 3 cases. I’ll show some variety in a different diagnostic entity within this category of SM [systemic mastocytosis]. This is a 68-year-old female. The patient had polymyalgia rheumatica, and then the patient presented with respiratory distress. If you see the CBC [complete blood count], it’s actually not too bad. Anemic, but the WB [white blood] cells are slightly elevated, and the platelets are OK, with 9% eosinophils. No organomegaly. Tryptase was elevated because the patient’s in respiratory distress, like outside in a work-up for the tryptase. By this point, you’ve already seen some bone marrow histology that Dan has shown you. They are mostly spindle cells…mast cells. Where these cells are very different, in contrast to what you have seen in a typical systemic mastocytosis, is that these spindle cells are very round. Here, it’s a typical mast cell, but these cells still contain some granules. However, they are very big, very roundish, and then morphologic-wise, they even look a little bit anaplastic. Here, to show you in higher power, these cells have a very prominent…so they don’t really look like a conventional, low-grade SM you may have seen. On the aspirate smear, the cells came out, so you can see, like Dan had shown in a couple of cases, more than 30% infiltration. But on the bone marrow aspirate smears, a lot of times, you only get probably 5%, or sometimes even less than 5%, because mast cell infiltration is usually associated with a lot of underlying fibrosis. They just don’t come out on the bone marrow aspirate smear. That’s also poignant.
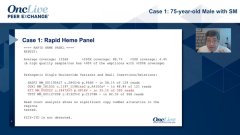
Why do you need high-sensitivity PCR [polymerase chain reaction] to do the KIT assay? Because the cells do not come out on the aspirate smear. You send a bone marrow aspirate smear; typically, you only have very low mast cells in the aspirate. But this case is a bit different. First of all, the cell is very ugly. It is, say, anaplastic looking. Another thing is, they do show on the bone marrow aspirate smear. Also, they are more than 20% of total cells. This is our flow cytometry. Not only did we do the CD117-positive cells, and because they are…negative…we also did a double gate. You can see the cells expressed CD2, CD30, and CD25. Also, they are located at the 45 upright…corresponding to, because they have all the granules. These are the immunohistochemistry scans. This is c-kit. Both are tryptase. You can see the mast cells expressed variably in the tryptase, where some cells are very strong, and some cells are much weaker for the tryptase. The karyotype came back and was normal. Actually, the KIT mutation was negative also, but these cells…more than 20% on the bone marrow aspirate smear, so there’s not a sensitivity issue here. This patient is negative for KIT D816V but positive for TET2.
These cells, by the pathology diagnosis for the criteria for mast cell leukemia; so the only diagnostic criteria required for mast cell leukemia is more than 20% mast cells on the bone marrow aspirate smears. We kind of question whether this definition is valid, why a lot of patients with 60%, 70% infiltration, they don’t come out on the aspirate smears because of fibrosis. We don’t call those mast cells leukemia. But when they have on the bone marrow aspirate smears, then we call it mast cell leukemia, even though they don’t have…mast cells. A lot of them are leukemic. The KIT D816V mutation is less frequent, but they may have a mutation among…KIT mutation. They may be sensitive to a tyrosine kinase inhibitor, or imatinib. CD2 and CD25 are frequently negative. Cells are often round, immature or anaplastic rather than spindly, and they may have accumulated other mutations.
Transcript edited for clarity.
Advertisement
Related Content
Advertisement

Latest CME

































Advertisement
Advertisement
Trending on OncLive
1
Single-Center, Retrospective Data Show Low Rate of Lifileucel Infusion Following Referral in Advanced Melanoma
2
Outcomes With Bridging Therapy Correlate With Cilta-Cel Efficacy, Safety in Multiple Myeloma
3
Real-World Data Support Clinical Benefit With Lifileucel in Previously Treated Advanced Melanoma
4
Long-Term Cilta-Cel Data Show Low Rates of PFS Events in Standard-Risk R/R Myeloma
5