

|Videos|August 23, 2021
Case 2: 46-year-old Woman With SM
Dan DeAngelo, MD, PhD, presents the case of a 46-year-old woman with systemic mastocytosis and associated gastrointestinal symptoms.
Advertisement
Episodes in this series

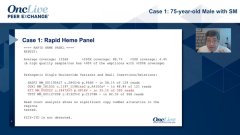





Dan DeAngelo, MD, PhD: Let me bring on a second case. She’s a wonderful woman. Ashley was referred about 15 or 16 years ago to me because she was in hospice care, believe it or not. She was being managed locally. She was having chronic diarrhea, weight loss, and abdominal distention to the point that she weighed about 40 kg. She had an indwelling catheter for TPN [total parenteral nutrition]. That’s how I inherited her. Her numbers had a tryptase of 770 ng/mL with a histamine level through the roof. CT [computed tomography] scan showed just dense ascites and hepatosplenomegaly. She had esophageal varices and gastric erythema, so there was evidence of portal hypertension, and a colonoscopy that showed pan-colonic edema with cecum, ascending transverse and descending colon throughout. Transjugular liver biopsy showed an elevated gradient. Marrow had more that 30% mast cells.
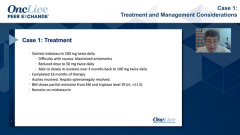
One of the things I wanted to bring to your attention are some of the GI [gastrointestinal] symptoms in mast cell disease. It’s highlighted in this particular case. I’ve highlighted her issues in red as she presented. But patients can have GI involvement of their mast cell disease and often get misdiagnosed as irritable bowel disease or other types of colitis. They present with abdominal pain due to gut motility or diarrhea, nausea due to some hyperacid secretion or delayed stomach emptying, vomiting from the same process sometimes from organomegaly but sometimes delayed emptying. Peptic ulcer disease, which is not uncommon in these patients because of the elevated histamine. This particular individual’s history was through the roof. GI bleeding due to histamine-induced acid secretion. Weight loss and malnutrition due to mast effect, the mast cell infiltration impeding normal gut absorption. Consequently, she really manifested many of these problems. These are just highlights of her histopathology.
This is a low power view of the H&E [hematoxylin and eosin] of her bone marrow. Here’s a bone marrow biopsy showing a KIT stain, the CD117. This is a tryptase, and this may highlight what Dr [Sa] Wang had mentioned. The CD117 is highlighting the vast majority of the mast cells vs tryptase, which is highlighting only a few. Because some of these are so dysregulated, they’re no longer staining tryptase. This is aberrant CD25, highlighting the bulk. Then this is a small intestinal biopsy from this patient, and I would argue that with H&E at this low power, you’re not able to see anything. I’m not a pathologist, but even at high power, I couldn’t tell you. There seems to be too many cells in the micrograph. But when you do the CD117 stain, you see that those cells are mast cells. There are a lot of mast cells in this GI biopsy, and they do stain for tryptase.
Transcript edited for clarity.
Advertisement
Related Content
Advertisement

Latest CME

































Advertisement
Advertisement
Trending on OncLive
1
Single-Center, Retrospective Data Show Low Rate of Lifileucel Infusion Following Referral in Advanced Melanoma
2
Real-World Data Support Clinical Benefit With Lifileucel in Previously Treated Advanced Melanoma
3
Long-Term Cilta-Cel Data Show Low Rates of PFS Events in Standard-Risk R/R Myeloma
4
Dr Riedell on the Long-Term Efficacy of Tisa-Cel in R/R Follicular Lymphoma
5