

|Videos|August 23, 2021
Case 2: Treatment and Management Considerations for SM
The panel of experts in SM discuss the diagnosis and management of a 46-year-old woman with systemic mastocytosis.
Advertisement
Episodes in this series

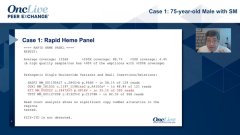
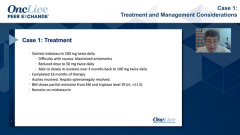





Dan DeAngelo, MD, PhD: This woman was started on midostaurin, and she did great for 12 years before she progressed. We were able to wean her TPN [total parenteral nutrition]. She went back to work and off hospice, and her GI [gastrointestinal] symptoms resolved. She was the poster child for our prior story on midostaurin. But after 12 years on midostaurin, she slowly developed—over a year and a half, it wasn’t rapid—more GI complaints, more ascites, more hepatomegaly, tryptase was going up. Then we rebiopsied her, and she was able to enroll in our PATHFINDER study. Prithviraj, I’ll start with you as my [fellow] hematologist here. What are your thoughts on this particular illustrative case?
Prithviraj Bose, MD: It’s incredible. It must be so gratifying to having cared for a patient like this. I mean, with the whole hospice transformation.
Dan DeAngelo, MD, PhD: It adds a little to the story, but it’s a true part of the story.
Prithviraj Bose, MD: I’m certain that it is. Also, the duration of response to midostaurin is very impressive. I know you published on the long-term outcomes of the midostaurin. That was phase 2. You said the patient is on PATHFINDER, and I presume she has responded. But there are multiple C findings, so ascites and splenomegaly. I forget her counts. I’m not sure.
Dan DeAngelo, MD, PhD: Her counts were OK. I forget what they were. I didn’t include that. She was anemic, but I don’t know if that qualified for a C finding. I can’t remember if it was less than 10.
Prithviraj Bose, MD: Right. But clearly the ascites, lots of edema all over, lymphadenopathy, and the organomegaly. A remarkable case.
Dan DeAngelo, MD, PhD: Dr Wang, I tried to highlight a few immuno-peroxidase studies. Any thoughts?
Sa Wang, MD: Yes, I agree. The GI biopsy—we say it’s so subtle. If you don’t think about this disease, you absolutely miss it. As you said, in the mucosa you always have a lot of cells. Also, you have nonspecific inflammatory response. You’re going to have increased…response cells, lymphocytes, and even eosinophils. You can have some allergy reaction. This patient does, when I saw your slides it has a lot of eosinophilia. Sometimes we look for mast cells because the eosinophilia and the mast cells go side to side.
Dan DeAngelo, MD, PhD: I’m not aware of that. If somebody has not just peripheral eosinophilia but eosinophilia in the tissue, then you’ll think about mast cells?
Sa Wang, MD: Yes. It’s kind of interesting. Sometimes the mast cell aggregates in the bone marrow. It can see the periphery of the mast cell…have a lot of eosinophilia. That’s the time, so some mast cells are probably in here. We start to look for mast cells because they come from the same precursors. There’s 1 type of the SM [systemic mastocytosis]...and that’s another common association with slightly increased eosinophils.
Prithviraj Bose, MD: Let me ask a question. This is independent of PDGFRA and FIP1L1 right?
Sa Wang, MD: Yes, we’re not talking about the 1 like…rearrangement, and then they can have increased eosinophils. Usually they aren’t forming SM, and occasionally they can present as SM. Whether they always have…mast cells, they’re scattered in the bone marrow.... They also often have CD25 expression. If the predominant presentation is hypereosinophilia, then with upper mast cells we have to rule out the PDGFRA arrangement. Also, in patients who we said presented with SM, if you really can’t find a KIT mutation, that’s also the time we start looking for this recurring arrangement.
Transcript edited for clarity.
Advertisement
Related Content
Advertisement

Latest CME































Advertisement
Advertisement
Trending on OncLive
1
Single-Center, Retrospective Data Show Low Rate of Lifileucel Infusion Following Referral in Advanced Melanoma
2
Long-Term Cilta-Cel Data Show Low Rates of PFS Events in Standard-Risk R/R Myeloma
3
Real-World Data Support Clinical Benefit With Lifileucel in Previously Treated Advanced Melanoma
4
Dr Riedell on the Long-Term Efficacy of Tisa-Cel in R/R Follicular Lymphoma
5