

|Videos|August 30, 2021
PATHFINDER Trial Efficacy Data
Dan DeAngelo, MD, PhD, reviews key efficacy data from the phase II PATHFINDER study.
Advertisement
Episodes in this series

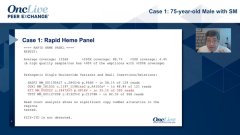
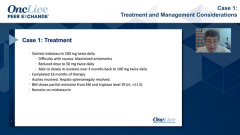





Dan DeAngelo, MD, PhD: Let me proceed on to just the PATHFINDER story, which I think is a new emerging data. Dr. Bose and I are both co-authors. This is the phase II data that was presented at the AACR [American Association for Cancer Research Meeting]. Just to remind you, this is a registrational phase II study where 60 patients were enrolled, all based on central pathology review. One of the things I think that Dr. Wong had brought up is that this is not an easy diagnosis. One of the things that we learned from the phase I study is that there were some patients who were enrolled as having a systemic mast cell cytosis that actually, on central review, didn’t. Here, we required central review, so everybody had a diagnostic thing. And whether they had C-findings or not, they were allowed to enroll. Only the C-findings were obviously evaluable for an end point because those are the C points that you can measure. These patients were all started at a dose of 200 [mg]. Initially, all patients were enrolled, but we ended up excluding patients who had platelets less than 50, and that was an amendment in 2019.
Just to go through some of the data at a high level, the overall response rate at this 200 milligram dose level was 75%. It’s a little shorter follow-up from the phase II EXPLORER study, but about 20% of patients had a complete remission and 30% of patients had a partial remission. The overall CR/PR [complete response/partial response] rate was 50%. And then, another group of the patients had clinical improvement, 25% of patients. Clinical improvement means that their C-finding improved or resolved, which for most patients is why they’re referring to you. You want to make a patient feel better.
The interesting thing about this study is that responses were seen regardless of the histologic subtype. Although responses seem to be highest, smaller number of patients, in the aggressive pure SM [systemic mastocytosis] versus the SM-AHN [systemic mastocytosis with an associated hematological neoplasm] because, again, there you’re dealing with the second component. The mast cell leukemia seemed to have the lower response rate. Responses were relatively equivalent regardless of whether patients were previously exposed to midostaurin [Rydapt], like the case I showed you, or whether they were midostaurin naive, and whether this was an initial treatment. One of the things that we like to do in oncology, of course, is we want to treat the disease so that patients can be cured if there’s a possibility. One of the important features to our job is to make patients feel better. I think we’re all in agreement with that.
Here, you can see this significant rapid reduction in their total symptom score. This is a symptom score. It’s a little bit different than the symptom score that’s used in myeloproliferative neoplasm, like myelofibrosis. But it’s similar. And here, you see a marked reduction in symptom score, and if you take the symptom score by specific entity, like fatigue, abdominal pain, skin lesions, pruritus, GI [gastrointestinal] toxicity, nausea, vomiting, diarrhea, you can see now, not every patient had one of these symptoms, but all of these symptoms improved in patients who had them. Thus, I think that that is just an important observation.
Transcript edited for clarity.
Advertisement
Related Content
Advertisement

Latest CME

































Advertisement
Advertisement
Trending on OncLive
1
Single-Center, Retrospective Data Show Low Rate of Lifileucel Infusion Following Referral in Advanced Melanoma
2
Real-World Data Support Clinical Benefit With Lifileucel in Previously Treated Advanced Melanoma
3
Long-Term Cilta-Cel Data Show Low Rates of PFS Events in Standard-Risk R/R Myeloma
4
Dr Riedell on the Long-Term Efficacy of Tisa-Cel in R/R Follicular Lymphoma
5