

|Videos|August 16, 2021
Case 1: Treatment Algorithm and Supportive Care Recommendations
Patricia Lugar, MD, MS, shares treatment algorithm and supportive care recommendations for a 75-year-old man with systemic mastocytosis.
Advertisement
Episodes in this series






Dan DeAngelo, MD, PhD: Dr Lugar, this patient clearly had systemic disease, so as an oncologist, I think he needs a cytoreductive therapy, but that doesn’t mean that this patient doesn’t still have SM [systemic mastocytosis]. He was having symptoms from recurrent urticaria pigmentosa and hives, allergic reactions, diarrhea. He was still having symptoms of his systemic mastocytosis. What’s a treatment algorithm that you would recommend in terms of supportive care for some of these patients who are not high-grade anaphylaxis but are having symptoms? What would you do?
Patricia Lugar, MD, MS: That’s interesting because the patients who are so advanced, like this man was in the first case, tend not to have as much presentation of what we consider a normal mast cell. These mast cells are a little different. They’ve matured out of their normal function, so we tend not to see as much anaphylaxis in reactivity or responsiveness. They’re more interested in interacting with the T cell, with other immune cells, and lose some of their normal function. It can be the people who have a tryptase of 25 ng/mL or 45 ng/mL that have a high burden of symptoms. For that, we don’t have too much to offer, and that’s why it’s exciting to be in the realm of other therapeutics: we always start with antihistamine therapy, and we look at mast cell stabilizers. Our usual regimen is antihistamine and mast cell stabilizers. You can look at leukotriene modifiers, and we treat with aspirin. We’ve been using biologics such as omalizumab more recently. Some patients are on a cocktail of all those medications. That can help to some degree with the cutaneous manifestations. It can help with some of the constitutional symptoms, such as the brain fog and the fatigue. It might help a little with some bone pain. These patients are symptomatic from multiple organ systems, so most of our patients receive that whole cocktail, unless we have a more definitive therapy in mind. But that’s generally where we get started, and it’s more of an additive therapy.
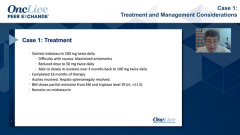
Dan DeAngelo, MD, PhD: I’m glad you mentioned that. This patient was on antihistamines as you mentioned, so both an H1 and an H2 blocker with cetirizine and famotidine. He was also on montelukast for a leukotriene stabilizer, and then he was started on steroids. That’s how I inherited him. With treatment of his disease, we were able to wean off the steroids, prednisone, and then we were able to wean off his montelukast. I was a little afraid about the H1/H2 blocker because he was doing well. That’s something, as we drove down his tryptase, that we could try. He wasn’t having anaphylaxis, so we had not escalated to a mast cell stabilizer.
Transcript Edited for Clarity
Advertisement
Related Content
Advertisement





Latest CME































Advertisement
Advertisement
Trending on OncLive
1
Single-Center, Retrospective Data Show Low Rate of Lifileucel Infusion Following Referral in Advanced Melanoma
2
Long-Term Cilta-Cel Data Show Low Rates of PFS Events in Standard-Risk R/R Myeloma
3
Real-World Data Support Clinical Benefit With Lifileucel in Previously Treated Advanced Melanoma
4
Dr Riedell on the Long-Term Efficacy of Tisa-Cel in R/R Follicular Lymphoma
5